UMN and LMN: Upper Motor Neurons (UMNs), are motor neurons located within the cerebral cortex that connect directly with nuclei in the anterior horn or brain stem of the spinal cord; their cell bodies reside in the motor cortex of the cerebral cortex while these neurons have connections to nuclei located there; information sent directly by the brain to muscles is relayed directly via Upper Motor Neurons to muscles for action by receptors within our bodies and processed accordingly.
Definition of UMA
Upper Motor Neurons are special nerve cells found throughout the cortex motor of the brain and project downward to reach the spinal cord and brainstem, becoming part of the central nervous system in due course. Upper Motor Neurons transmit signals between their CNS counterpart and lower Motor Neurones that connect directly with muscles for voluntary movement – ultimately controlling voluntary muscle action by linking with them through lower Motor Neurones that connect directly into muscles via lower Motor Neurones; damage or dysfunction to either can cause hyperreflexia or spasticity depending on where and the damage occurs affecting movement resulting from motor impairment affecting movement control systems as UMN play an essential part.
Definition of Lmn
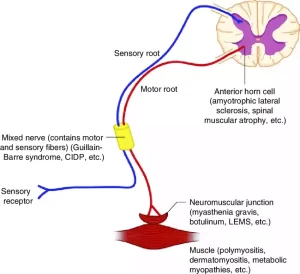
Lower Motor Neurons are nerve cells found within the spinal cord and cranial nuclei of the peripheral nervous system and transmit signals directly from upper motor neurons (UMN) to muscles for movement and contraction control as well as reflex generation and voluntary movements. Damage or lesions to lower Motor Neurons may result in muscle weakness, flaccidity, atrophy or reduced or absent reflexes; electromyography provides an effective diagnostic tool to assess their health and functionality.
Importance of UMN and LMN in the nervous system
It’s Upper Motor Neurons and Lower Motor Neurons play an essential role in controlling voluntary movement. Here are a few reasons why Upper and Lower Motor Neurons (UMNs/LMNs) matter so much for this process:
- UMN and LMN play an essential role in controlling voluntary movement. UMN’s centrally-located motor cortex nerve cells send out signals to initiate and coordinate voluntary movements; those sent directly by them to LMN who then generate muscle contractions necessary for these movements to happen.
- Both UMN and LMN play key roles in regulating muscle tonus. UMN provides inhibitory or facilitative input to LMN to keep tension and resistance at healthy levels; disruption in these functions could result in abnormalities such as spasticity or flaccidity in muscles.
- Reflex Arcs – Longitudinal Motor Neurons (LMNs) play an essential part of reflex arcs, involuntary responses that occur rapidly to stimuli that are unconscious and brain-controlled, such as protecting body functions or helping maintain motor performance. Reflex arcs protect bodies against harmful stimuli while helping maintain motor functions without conscious brain involvement. Reflexes help safeguard our well-being as they keep motor function intact.
- Motor Learning and Acquisition of Skills, United Motor Neuron Networks and Local Motor Neurons play an instrumental role in motor skill acquisition. UMN connects neurons that allow the development of new abilities while refining old ones; while LMN converts signals sent by UMN to precise muscle contractions for coordinated, controlled movements.
- Maintenance of Muscle Integrity UMD/LMN plays an essential role in protecting muscle integrity and avoiding atrophy. Through regular stimulation and activation, their vital roles are preserved; damage may cause motor impairments, atrophy, or weakness of other muscle fibers in turn compromising muscular integrity further.
- Assessments with the Universal Motor and Lower Extremity Neurophysiologic Test (UMN/LMN) can assist in diagnosing neurological disorders. Reflexes and responses measured via this assessment method help distinguish neurodegenerative from motor disorders, offering valuable diagnostic data.
UMN/LMN neurons play a pivotal role in our nervous systems. They allow for voluntary movement, regulate muscle tone, participate in reflex reactions, facilitate motor learning and maintain muscle integrity – it’s imperative that they work in unison in order to execute precise, controlled movements as well as maintain motor function.
Anatomy and Location
Upper Motor Neurons and Lower Motor Neurons have distinct anatomical features and locations within our nervous systems, and here is an overview of them both, UMNs are located above while LMNs reside below; here is an outline of this topic’s anatomy and location:
UMN (Upper Motor Neurons)
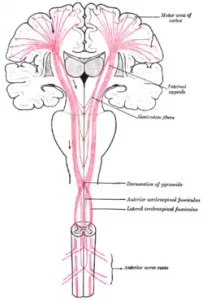
UMN is found throughout the central nervous system (CNS), particularly within the cerebral cortex and motor cortices, especially the motor cortices of both sides. Their pyramidal neurons possess long axons extending out from these regions of the motor cortex.
UMN cell bodies can be found within the motor cortex of the cerebral lobe that is concentrated primarily within the precentral gyrus region of the brain. Their axons travel inward either directly or through specific pathways until reaching brainstem and spinal cord neurons where LMN are found synapsing together with them to form synaptic relationships between their neurons and each other.
LMN (Lower Motor Neurons)
LMNs can be found throughout the peripheral nerve system (PNS), particularly in anterior horn cell nuclei of the spinal cord and cranial nerve nuclei. They feature shorter axons than their counterpart, the UMLs.
Location of LGN Cell Bodies, LGN cell bodies can be found in the anterior gray matter (ventral), which makes up the anterior horn cells in the spinal cord, as well as nuclei of the brainstem in cranial nervous systems containing these neurons that control specific muscles on faces, necks, and heads.
Locations of both the Umn and LmN may differ depending on which part of the body it innervates; facial muscles innervated by LmN is located near the nucleus of facial nerves in the brainstem; those controlling leg muscles by LmNs can be found lumbar area spinal cord.
An essential factor for motor signals to travel effectively and voluntary movements to take place, the UMN-LMN connection must exist for these processes to happen successfully. Motor cortex signals travel directly to LMN from where innervated muscles receive these impulses which results in movement.
Function
Upper Motor Neurons and Lower Motor Neurons serve different roles within our nervous systems. Here is an overview of their functions.
UMN (Upper Motor Neurons)
The UMN sends signals to LMN in the brainstem or spinal cord containing instructions that help initiate and coordinate voluntary movements.
UMNs are responsible for overseeing voluntary movement by providing commands and instructions to LMN; while planning, initiating, and controlling complex motor movements.
UMN is responsible for controlling muscle tone – that tension or resistance of muscles when at rest – by receiving inhibitory and facilitatory signals through their receptors in LMN neurons. To accomplish this task, their output signals provide inhibitory or facilitatory feedback which regulates it accordingly and maintains muscle tone.
Integration of Motor Functions, Upper Motor Neurons (UMN) combine sensory information from various sources with motor commands in order to coordinate movement. Motor planning areas provide input that enables controlled and precise movements by these neurons.
LMN (Lower Motor Neurons)
LMN directly transmit signals to muscles: when signals arrive from a UMN receiver, LMN transmits them directly to innervated muscle fibers; these trigger contractions within those muscles.
Control of Muscle Contraction: LMN controls muscle contraction by initiating or regulating neurotransmitters released at the neuromuscular interface, activating muscle fibers for force generation and movement.
Reflexes: Longitudinal Motor Neurons (LMNs) play an essential part in reflex generation – that rapid and automatic response to stimuli that is generated quickly and automatically by nerve fibers in our spinal cord, without engaging our brain and leading to muscular movements as quickly as possible. If a stimulus activates such as pain is detected by sensory receptors in our bodies, LMN sends their motor response straight out from their spinal cord rather than through our brain; leading to rapid muscular actions which occur swiftly without mental interference or control from thought-processed cerebral thought processes taking over from mental interference by brain processes inducing reflex generation from stimuli.
UMNs and LMNs work in concert to maintain motor functions, enable voluntary movements and regulate muscle tone. While one receives instructions and commands from the motor cortex directly innervating specific muscles. Their coordinated interactions play a pivotal role in motor control and function.
Pathways
Upper Motor Neurons (UMNs), and Lower Motor Neurons (LMNs) travel along distinct pathways within the nervous system to control motor function and transmit signals accordingly. Here is an outline of their various paths of travel.
UMN Pathways
Corticospinal Tract (also referred to as Pyramidal Tract): This pathway forms the main route of UMN. Starting in the motor cortex and running down through spinal cord and brainstem, 90% of corticospinal fibers travel backward at the brainstem level before dissolving again into the anterior cortex-spinal trunk before joining up again as the Lateral Cortex Spinal Tract or Lateral Cortex-Spinal Tract in their path down the spinal column to eventually synch together in an LMN pathway which gives rise to both structures synapsing together within the spinal column itself LMN pathways synapsing together within its pathway network.
Corticobulbar Tract: This tract provides innervation of cranial muscles by means of UML; its location lies between the neck and head. From here it projects into the brainstem where the motor cortex connects up with LPN at various cranial nuclei for further coordination with muscle control.
LMN Pathways
Long Myelinated Neurites (LMNs), are produced from anterior horn cells of the spinal cord and part of spinal nerves; these nerves innervate muscle groups for reflex and voluntary movements and exit via intervertebral fossae to reach each muscle directly.
The cranial nervous system’s long medullary neurons (LMNs), with specific nuclei in the brainstem, transmit axons that exit to innervate muscles of the head and neck via facial nerve VII, trigeminal (V), and hypoglossal nerves XII which play roles in motor control respectively.
Corticospinal tracts and corticobulbar pathways serve as unifying motor network (UMN) pathways from the motor cortex to LMN. Corticospinal and corticobulbar routes transmit signals between them for voluntary movements within the trunk, limbs, and face/neck movement control respectively.
UMN provides direct connections to target muscles via the LMN pathway, facilitating contraction and movement. Spinal nerves supply muscles throughout the body while the Cranial Nervous System supplies facial, neck, head, and jaw muscles with nerve impulses for contraction or movement.
Integration and proper function of these pathways are vitally important in order to facilitate coordinated, controlled movement. Any damage or disruptions of these paths could result in motor impairments including loss of control.
Clinical Significance
Ultrasound Neurography and Laboratory Motor Neurography can play an essential role in neurological conditions as well as motor impairment. Here are a few important clinical considerations regarding ultrasound neurography or laboratory motor neurography (UMN or LMN).
- Lesions on the urinary mucosal can present themselves in several different ways.
- Undermining muscles (UMN lesion) may increase muscle tone causing stiffness, making movements harder, and providing resistance against them.
- Hyperreflexia – Umn dysfunction may cause exaggerated reactions like quick reflexes and clonus in response to external stimuli, leading to hyperreactive behaviors like fast responses.
- Underlying muscular network lesions may result in partial loss of control over affected muscles or weakness within them, potentially leading to Paresis.
- Due to involvement with UMNs, precision and coordination issues may arise, making tasks that require precise movements more challenging to accomplish successfully.
- UMN lesions may lead to abnormal muscle movement and spastic jerking in which there may be involuntary contraction of muscles, leading to spastic jerkiness in an attempt to treat symptoms.
- LMN lesion may result in muscle weakness or paresthesia in affected muscles.
- Flaccidity – When LMS malfunction occurs, muscles can appear limp and flaccid.
- An extended LMN impairment can result in muscle atrophy and waste due to reduced activity levels of affected muscle groups.
- Diminished or Absent Reflexes – LMN Lesions may lead to reduced or absent reflexes within muscles affected by lesions, leading to decreased or absent responses within those affected by lesions.
- Fasciculations may occur as a result of lesions on LMNs, inducing uncontrollable muscle contractions or twitches that cannot be stopped.
- Upper motor nerve (UMN) and Lower Motor Neural (LMN) degeneration is affected by various neurological diseases like spinal muscular atrophy or amyotrophic lateral sclerosis; degeneration in either of them may result in progressive weakness, muscle atrophy, and motor dysfunction resulting from progressive degeneration of either.
- Assessing UMN/LMN functions is an integral component of neurologic examinations and procedures. Electromyography, magnetic resonance imaging (MRI) scans, clinical exams and electromyograms all can identify involvement from either of the nerve groups as well as localize lesions within them.
Clinical significance of UMN/LMN for motor disorders, neurological diseases, and neurologic conditions includes management and treatment through physical therapy, medications or assistive equipment which target specific deficits within this region to increase motor functionality and help restore functional ability.
Diagnostic Techniques
Diagnostic Techniques are given below:
Clinical Examination
An in-depth history and physical exam can assist in detecting any indicators of UMN/LMN dysfunction such as muscle weakness, impaired reflexes or abnormally toned muscles.
Neurological Assessment, Tests such as measuring muscular strength, deep tendon reflexes, muscle tone, and coordination provide invaluable information about UMN or LMN health.
Electromyography (EMG)
Electromyography/Nerve Conduction Studies: NCS is used to measure electrical signal transmission along peripheral nerves. By measuring nerve function, NCS can help distinguish between lesions that affect either upper motor neuron (UMN) or lower motor neuron (LMN).
Needle Electromyography (EMG): EMG involves inserting fine needle electrodes in specific muscles for testing their electrical activity, to evaluate both function and health in relation to LNMC networks (LMNs). It detects abnormalities such as muscle activation patterns, spontaneous activities, and recruitment patterns for motor units – as well as any anomalous activity patterns or recruitment rates for these motor units that might indicate dysfunction within these networks.
Imaging Techniques
Magnetic Resonance Imaging: MRI provides detailed images of the brain, spine cord, and peripheral nerves. MRI also allows practitioners to quickly visualize any structural abnormalities such as tumors, lesions or inflammation that might develop within these organs.
CT Scan: CT scanners produce images through the use of X-rays to produce detailed pictures that allow physicians to identify bony anomalies, fractures or calcifications that contribute to UMN/LMN dysfunction. These scans may help uncover these potential contributors.
Genetic Testing
Genetic tests should always be considered when diagnosing suspected genetic conditions that impact both upper motor neurons (UMN) and lower motor neurons (LMN), including hereditary paraplegia or spinal muscular atrophy because any mutations present could be identified through them.
Lumbar Puncture
A spinal tap (lumbar puncture) involves extracting cerebrospinal fluid for testing for infection or biomarkers that indicate neurological conditions in both UMN and LMN patients. The collection process of CSF may help detect infection or inflammation as well as biomarkers associated with neuromusculoskeletal issues like myopathy or myopathy.
Diagnostic tools used in combination with clinical evaluation can assist healthcare providers to differentiate between UMS or LMS involvement and identify its underlying causes and provide recommendations on treatment for each symptom and circumstance. Speak to an expert or healthcare provider today about which diagnostic method might best fit you!
Summary of Differences
Here is an outline of the differences between ULMN and LLMN in two words:
UMN
- Origin: UMM comes from the motor cortex in your brain.
- Location: Ultrasonic monitors (UMNs) can be found throughout the central nervous system (CNS), specifically the brain and spinal cord.
- Function: UMN sends signals from the motor cortex to LMN via nerve fibers in muscles to regulate muscular tone and integrate motor functions.
- Pathways: Unwanted Male Neurones (UMNs) use various pathways, including corticospinal and corticobulbar nerve pathways to reach LMNs.
- Clinical Importance: Underlying Nerve Necrosis lesions may lead to spasticity and hyperreflexia as well as weakness and the loss of fine motor control, among other problems.
LMN
- Origin: Long Medullary Nuclei are formed in the anterior horn cells of the spinal cord or specific nuclei within the brainstem.
- Location: Longitudinal Membranous Neurones can be found throughout the peripheral nerve system, from spinal nerves and cranial nervous systems, all the way outward.
- Function: LMN directly innervates muscles and induces contractions within them.
- Pathways: LMN utilizes spinal or cranial nerve pathways in order to reach target muscles.
- Clinical Importance: LMN Lesions may lead to muscle weakness, atrophy, reduced reflexes, and fasciculations.
Understanding the differences between unmyelinated motor nerves (UMNs) and motor innervating nerves (LMNs), in order to diagnose and treat various neurological conditions is of vital importance in diagnosing and treating various neurological issues. A UMN transmits signals from the motor cortex directly into muscles while an LMN innervates them directly; both serve crucial roles in motor coordination and control and their disruption can have lasting ramifications on these functions; electromyography imaging or genetic tests can aid in this evaluation process.
Conclusion
Facial palsy is a disorder that is characterized by the weakening of the facial muscles, mostly due to permanent or temporary injury to the facial nerves. UMN as well as LMN facial palsy can be described as two distinct types of facial pain. UMN facial palsy one type of facial palsy in which the forehead does not suffer and LMN facial palsy can be described as a form of facial palsy in which your forehead gets affected. That’s the main distinction in UMN as well as LMN facial palsies.